
Many patients who present to the dermatologist are found to have systemic problems, and conversely, dermatologists are often called in to consult on patients with systemic diseases with cutaneous manifestations. Psoriatic arthritis is perhaps the most familiar example of a disorder with dermatologic and rheumatologic manifestations and a single underlying pathology.
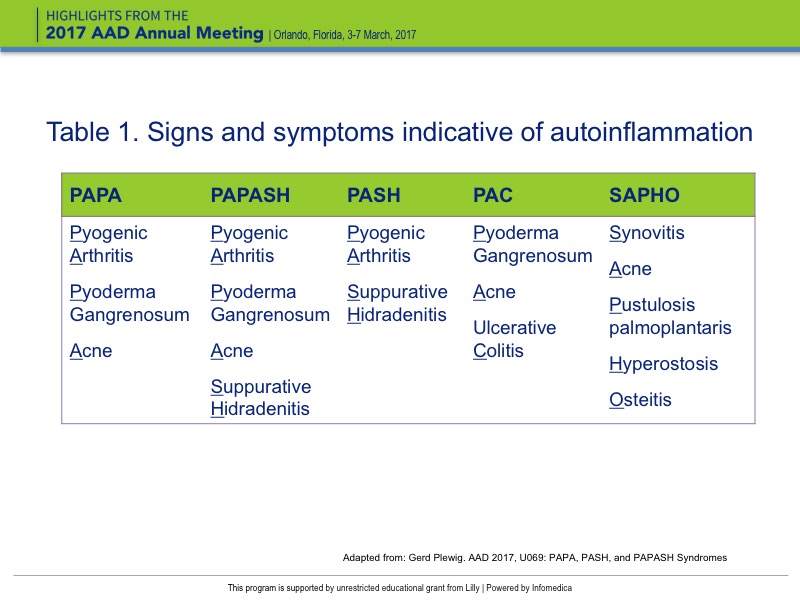
A group of dermatologic syndromes were discussed by Prof. Gerd Plewig, Dept. of Dermatology, University Munich, Munich, Germany including acne fulminans, hidradenitis suppurativa , SAPHO (synovitis, acne, pustulosis palmoplantaris, hyperostosis, osteitis), PAPA (pyogenic arthritis, pyoderma gangrenosum, acne), PASH (pyoderma gangrenosum, acne, suppurative hidradenitis), PAC (pyoderma gangrenosum, acne, ulcerative colitis) and PAPASH (pyogenic arthritis, pyoderma gangrenosum, acne, suppurative hidradenitis). These syndromes highlight important insights on the relationships between genetic mutations, inflammation, and disorders affecting connective tissue (Table 1). Most importantly, therapies targeting inflammation provide new hope for treating these disorders.
{kind=link}
These autoinflammatory diseases are often associated with genetic abnormalities which can be identified through genetic testing, if available. The culprit mutations identified thus far occur in genes that ultimately regulate inflammasomes. These are innate immune complexes that regulate the activation of caspase-1 and induce processing of the proinflammatory cytokine interleukin (IL)-1ß. Targeting IL-1ß has shown success in treating these diseases.
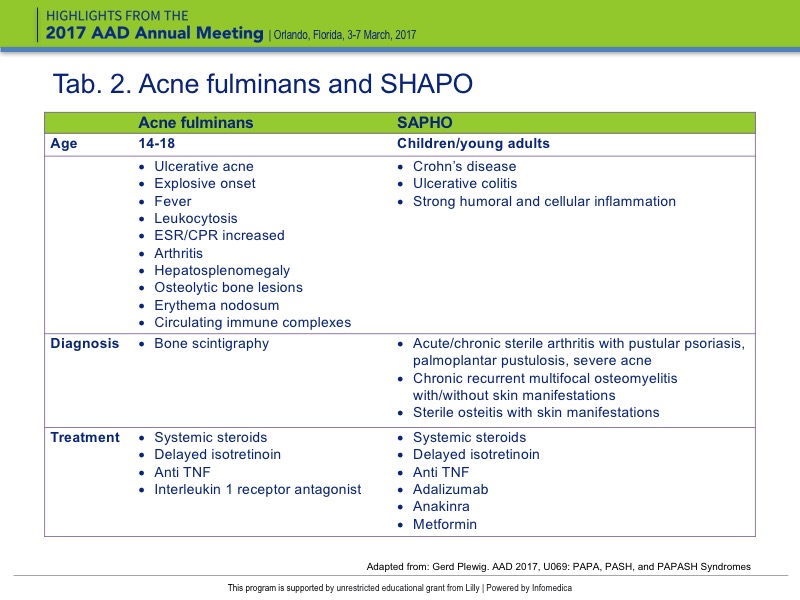
In particular, two diseases, acne fulminans and SAPHO, were discussed by Gerd Plewig (Table 2). Their symptoms can lead to multiple visits to different specialists, depending on either joint involvement or presence of skin lesions. Regardless of which specialist is seen, a clear overlap of symptoms is present. This fact necessitates the awareness of diseases by both specialists.
{kind=link}
Acne fulminans is characterized by ulcerative acne with an explosive onset, thus its name “fulminans” (Table 2). Males are primarily affected and may have fever, leukocytosis, elevated erythrocyte sedimentation rate (ESR)/C-reactive protein (CRP), circulating immune complexes, hepatosplenomegaly, arthritis, osteolytic bone lesions, and erythema nodosum. Patients are often between the ages of 14 to 18 and suffer from severe pain by the time they reach the medical office. Patients often prefer to stand over sitting, because of the associated pain, and if they do sit, it may take time for them to be able to stand upright again. Diagnosis and treatment of acne fulminans involves a bone scintigraphy, immediate initiation of systemic steroids, and use of isotretinoin at a later date. It is important not to initiate patients on isotretinoin, because early initiation can aggravate the disease.
SAPHO syndrome (Table 1) represents the spectrum of inflammatory bone disorders and, at first, patients may seek a rheumatologist for their joint pain.
When the rheumatologist sees lesions on the skin, dermatologists are often called in to consult, and at this point an accurate diagnosis can be made. SAPHO syndrome has two disease patterns: an inflammatory pattern and a bone remodeling pattern. It often presents in children and young adults, and may involve bowel conditions such as Crohn’s disease (CD) and ulcerative colitis (UC). SAPHO is characterized by strong humoral and cellular inflammation. Diagnosis can be made based on the presence of chronic recurrent multifocal osteomyelitis with or without skin manifestations, acute/chronic sterile arthritis with pustular psoriasis, palmoplantar pustulosis, severe acne, and sterile osteitis and skin manifestations. Patients should be treated with steroids and subsequently with isotretinoin.
Hidradenitis suppurativa (HS), sometimes referred to as suppurative hidradenitis and acne inversa, is an autoinflammatory condition associated with dissecting terminal hair folliculitis. Despite the name “acne inversa,” hidradenitis is not a form of acne, because it involves the terminal follicles rather than sebaceous follicles. It is characterized by the formation of abscesses with epithelial-lined channels, with formation of draining sinuses in the axillae, groin, buttocks area, and in women, under the breasts. Bacterial superinfection may occur, with foul-smelling secretions, as well as the development of dermal contractures. In some cases, squamous cell carcinoma (SCC) may develop, particularly in the anal folds, potentially leading to fatal metastases and death. In early stages, limited areas of disease can be surgically excised. Some research suggests that mutations in genes that encode key components of the gamma-secretase protein may be involved in its pathogenesis.
There is a strong association between inflammatory bowel disease (CD and UC) and hidradenitis suppurativa. In a 2010 study by Van der Zee et al. of 158 patients with IBD, the prevalence of HS was 16%; a 2014 study (van der Zee et al.) of 909 patients with IBD found a prevalence of HS presence in 23% of patients. IBD is typically managed with TNF-α inhibitors.
Over the last several years, researchers have identified additional syndromes characterized by clusters of signs and symptoms suggestive of autoinflammation, listed in Table 2.
These syndromes, along with SAPHO, are thought to be variants belonging to the clinicopathological spectrum of autoinflammatory diseases, characterized by an abnormal activation of innate immunity. These syndromes share a common etiology, which may involve mutations in the proline–serine–threonine phosphatase-interacting protein 1 (PSTPIP1) gene, resulting in increased binding affinity to pyrin, which facilitates assembly of inflammasomes.
All are likely to respond to agents that block IL-1 signaling. One such agent is anakinra, which has been successfully used in treating many of these disorders. Anakinra is a recombinant human IL-1β antagonist. It is indicated for the treatment of rheumatoid arthritis (RA) and cryopyrin-associated periodic syndromes (CAPS). However, its use in SAPHO, PAPA, PAPASH, PASH, and PAC is off-label. Adverse events (AEs) associated with anakinra include injection site reaction, headache, neutropenia, and bacterial infections. It is not, however, associated with activation of latent tuberculosis.
Canakinumab is another IL-1β blocker that may also have off-label use in these autoinflammatory syndromes.