
Systemic therapy for atopic dermatitis should not be taken lightly. Traditional topical agents, wet wraps, and emollients are a natural firstline option. However, there are times where more intensive therapy is required to remediate the disease, providing relief to the patient.
The patients’ quality-of-life should also be a main objective for initiation of systemic therapy. A dermatologist should ask quality-of-life questions to determine the patient’s need and impact of his or her condition. How is the patient’s psychological health? Is he/she depressed, is he/she able to sleep? What is the impact of the condition on school or work? Are patients able to participate in extracurricular activities? This information will provide a broader assessment of the patients aside from the clinical symptoms being presented.
Phototherapy falls under the category of systemic therapy. It is used as a second line therapy after first-line/topical agents fail. The ability of patients to respond to phototherapy may vary because of different circumstances. Some geographic areas are not conducive to phototherapy or some patients are too young to tolerate being in a phototherapy booth. Even more essential is the inability of many patients to attend multiple phototherapy sessions in a week because of time commitment, work, personal, or other constraints. All of these factors should be taken into consideration and discussed with the patient to see if incorporating phototherapy treatment is a viable option for that patient/family. It is noteworthy to mention, that there is some variability between national and global guidelines especially in the use of children. However, Heather Brandling-Bennett, associate professor of the Division of Dermatology, Department of Pediatrics in Seattle Children’s Hospital University of Washington School of Medicine, Washington, USA says that considerations to administer phototherapy at a young age should be made based on each individual patient. Some 5-year-old children can tolerate the therapy while a 10-year-old child will not. In some cases, a parent may accompany the child to encourage a more successful phototherapy session.
Focusing on other treatments, cyclosporine is an option for patients who are refractory to first line treatment with atopic dermatitis, albeit it is considered an off-label use in the United States. However, its use is widespread in other parts of the world such as Germany, France, Canada, and other European countries. It was also the most common first-line systemic therapy in a survey capturing US, Canadian, and European responses. Brandling-Bennett discussed her preference for cyclosporine use, because of its rapid response that provides almost an immediate relief for her patients. Cyclosporine is not a long-term option and it should be tapered after a few months with a goal of discontinuing cyclosporine therapy within 12 months after initiation.
Methotrexate is a systemic therapy that has shown favorability in atopic dermatitis patients. While a test dose is suggested in the guidelines, Brandling-Bennett noted that sometimes when test dosing in pediatric patients, the risk of losing patient confidence is increased as low dose treatments may not be effective. More robust dosing at initiation often works well in atopic dermatitis. Folic acid should be prescribed during methotrexate therapy and ondansetron may be used to limit anticipatory nausea and vomiting associated with methotrexate therapy.
Mycophenolate mofetil may be used in patients as well. However, it is also known to cause gastrointestinal upset. Initiating at guideline doses can be incorporated or may be titrated up over 2-3 weeks to minimize gastrointestinal adverse events and increase tolerability. Baseline and follow up labs are suggested for mycophenolate mofetil use, as well as, open discussion with regards to birth control and pregnancy. A REMS program is also associated with mycophenolate mofetil and should be adhered to.
Azathioprine is a systemic option but has a delayed effect of 12 weeks or more to show improvement. Surveys, both locally and abroad, show azathioprine used as a second or third line therapy after cyclosporine use. A comparison of each of the treatments can be reviewed in Table.
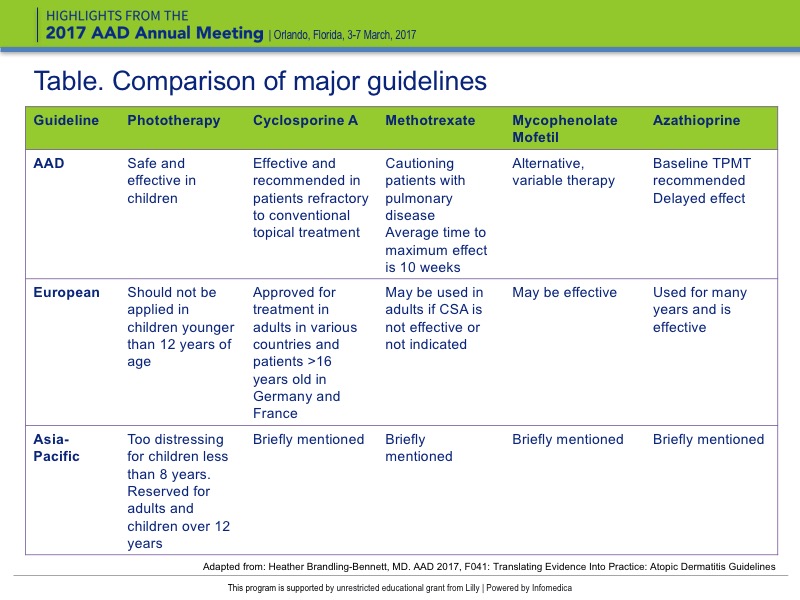{kind=link}